In this short article we’ll briefly explain what dysphagia is. We’ll also briefly describe the causes, incidence and effects of dysphagia.
What Is Dysphagia?
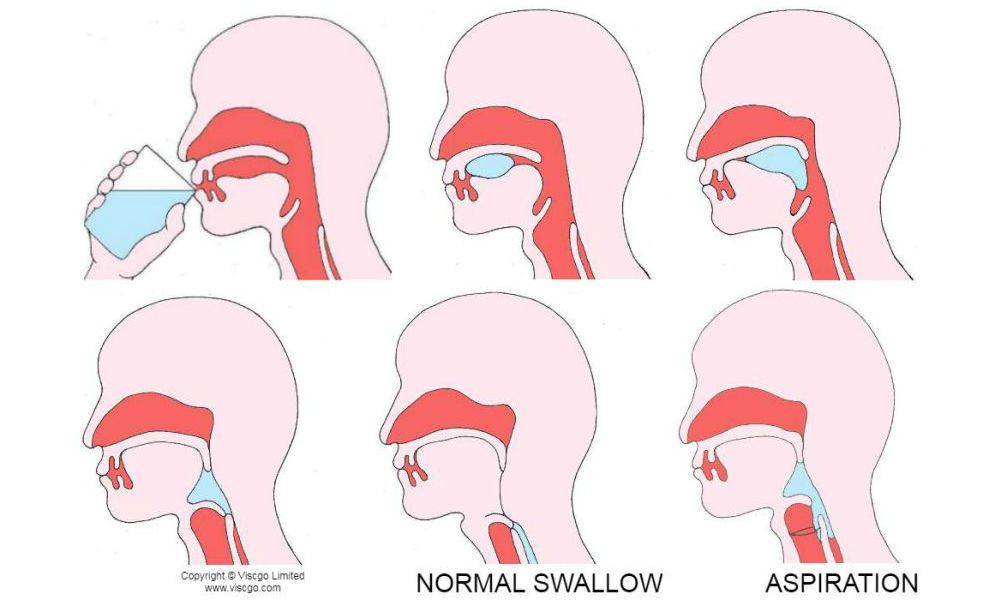
Dysphagia is the medical term for difficulty swallowing (also known as swallowing disorder or swallowing disability). Dysphagia comes from the Greek words “dys” which means disorder and “phagia” which means to eat.
Oropharyngeal dysphagia is caused by a swallowing disorder in the mouth or throat. Oesophageal / esophageal dysphagia is caused by a swallowing disorder in the oesophagus / esophagus (the tube that carries food from your mouth to your stomach). It can be mild or severe and can be short or long term.
What is dysphagia caused by?
The usual causes of dysphagia are nerve or structural damage which interferes with swallowing (moving food and drink safely from the mouth to the stomach). Consequently, swallowing difficulty is often a secondary condition of many other ailments, especially acquired neurological conditions and degenerative diseases such as:
- dementia, stroke, Parkinson’s disease, motor neurone disease, multiple sclerosis, cancer, age-related weakening of the muscles (common in elderly people)
- cerebral palsy, developmental conditions or learning disabilities in children from birth
- psychological disorders
- head injuries, complications resulting from head or neck surgery
- side effects of some medication such as sedatives, antidepressants, antipsychotics and chemotherapy
- chronic obstructive pulmonary disease and gastro-oesophageal reflux.
What is the incidence of dysphagia?
Dysphagia is estimated to affect 8% of the general population which is 560 million people worldwide. Swallowing disability can affect people at any age but is prevalent among the elderly, particularly following stroke and in the end stage of dementia. It affects:
- 40-78% stroke survivors1
- 68% of people with dementia in long-term care2
- 50-75% of nursing home residents3
- 50-60% of head and neck cancer survivors4
- 99% of children with acute cerebral palsy5
- the majority of people with progressive neurological diseases such as Parkinson’s disease and multiple sclerosis
- over 90% of people with motor neurone disease6.
The incidence of dysphagia is likely to increase for two reasons. Firstly, the global population as a whole is increasing. Secondly, people live longer now on average and it affects elderly people more.
What are the effects of dysphagia?
People with swallowing difficulty might experience problems with sucking, chewing and swallowing food and drink, controlling saliva and ingesting medicine. Dysphagia can cause pain, heartburn, hoarseness, coughing, regurgitation, a sensation of food stuck in the throat or chest, drooling, loss of appetite, food refusal, weight-loss, choking, malnutrition, dehydration, aspiration, pneumonia and death.
As you can see from the following quotations, swallowing difficulty can have a major impact on quality of life:
“The most feared complication of dysphagia after stroke is aspiration pneumonia.” 7
“33% with dysphagia after stroke suffer pulmonary infection.” 7
“Dehydration and malnutrition are also common in dysphagic patients.” 7
“49% of stroke survivors admitted to a rehabilitation unit were malnourished, and the malnutrition was associated with dysphagia.” 7
“58% of acute stroke survivors with dysphagia had signs of dehydration.” 7
“Dysphagia can adversely impact quality of life. Only 45% of patients with dysphagia find eating enjoyable, and 41% of patients with dysphagia experience anxiety or panic during mealtimes. More than 1/3 of patients avoid eating with others because of dysphagia.” 7
As well as adversely affecting the individual, dysphagia also has a significant effect on healthcare resources. For instance, in the US, the presence of swallowing disorder was associated with a 40% increase in length of hospital stay (an extra 1.64 days on average) at a cost of $2,454 a day. The conservative estimated annual cost of swallowing disorder due to this increased hospitalization is $547,307,964.8
In our next article we’ll look at dysphagia treatment and management.
What is your experience of / involvement with dysphagia? Please feel free to leave a response below.
References
- Martino R, et al. Dysphagia after stroke: incidence, diagnosis and pulmonary complications. Stroke 2005; 36(12): 2756-2763
- Feinberg MJ, et al. Deglutition in elderly patients with dementia: findings of videofluorgraphic evaluation and impact on staging and management. Radiology, 1992; 183(3): 811-814
- O’Loughlin G, and Shanley C, Swallowing problems in the nursing home: a novel training response. Dysphagia 1998; 13(3): 172-183
- Shune SE, et al. Association between severity of dysphagia and survival in patients with head and neck cancer. Head Neck 2012; 34(6): 776-784
- Calis EAC, et al. Dysphagia in children with severe generalized cerebral palsy and intellectual disability. Developmental Medicine & Child Neurology 2008; 50: 625-630
- Royal College of Speech and Language Therapists. Resource Manual For Commissioning And Planning Services For SLCN – Dysphagia. 2009
- Gonzalez-Ferrnandez M, et al. Dysphagia after stroke: an overview. Curr Phys Med Rehabil Rep. 2013; 1(3): 187–196
- Altman KW, et al. Consequence of dysphagia in the hospitalized patient: impact on prognosis and hospital resources. Arch Otolaryngol Head Neck Surg. 2010; 136(8): 784-789